


Rethinking independence as the primary benchmark for AAC success
Published on Jul 07, 2026

- The independence assumption in AAC goals and progress tracking
- The independence assumption in clinical decision-making
- Does AAC need to be used independently to be effective?
- Where does support-based communication thrive?
- Other measures of AAC effectiveness
- Rethinking goals, documentation, and success metrics
- A more nuanced view of AAC success
AAC success isn’t just about independence. Research shows supported communication drives better participation and outcomes — requiring a shift in how we define goals and measure progress.
The independence assumption in AAC goals and progress tracking
Raise your hand if one of your go-to AAC goals sounds like, “Patient will independently use AAC device to communicate basic needs.”
Now raise your hand if you measure progress by counting cues or documenting movement toward “independent” device use.

If you’re like most SLPs (hi!), independence has probably become your go-to benchmark for AAC success. It shows up in our goal writing, our progress documentation, and our clinical decision-making. For many of us, it’s what we were taught in grad school!
But what if we have it all wrong? Or…mostly wrong?
What if this focus on independence is limiting our understanding of what successful AAC use actually looks like?
Let’s pause, wipe the lens a bit, and take a clearer look at whether independence should be our primary benchmark for AAC success — and what research tells us about how communication really works in everyday life.
The independence assumption in clinical decision-making
If we’re honest, independence shows up everywhere in adult AAC practice. Consider how it shows up in your daily clinical work:
In goal writing:
- “Patient will independently navigate AAC device to express wants and needs”
- “Client will independently initiate communication using AAC across all environments”
- “Patient will demonstrate independent functional use of speech-generating device”
In progress notes:
- “Requires moderate cues to access AAC device”
- “Demonstrates improved independence with device navigation”
- “Continues to need maximal support for AAC use”
In clinical decision-making:
- Determining AAC candidacy based on potential for independent use
- Measuring therapy success by reduction in cueing needs
- Making discharge decisions based on achieved independence levels
- Justifying continued services by documenting movement toward independence
There’s this underlying assumption that independence equals success, while ongoing support suggests incomplete progress or even failure.
But when we look at who makes a good candidate for AAC devices, research shows there are no specific prerequisite skills required. This challenges the notion that independence should be a requirement or even an expectation for successful AAC use.
Does AAC need to be used independently to be effective?
While independence feels like a solid goal, research tells a different story about what makes AAC successful.
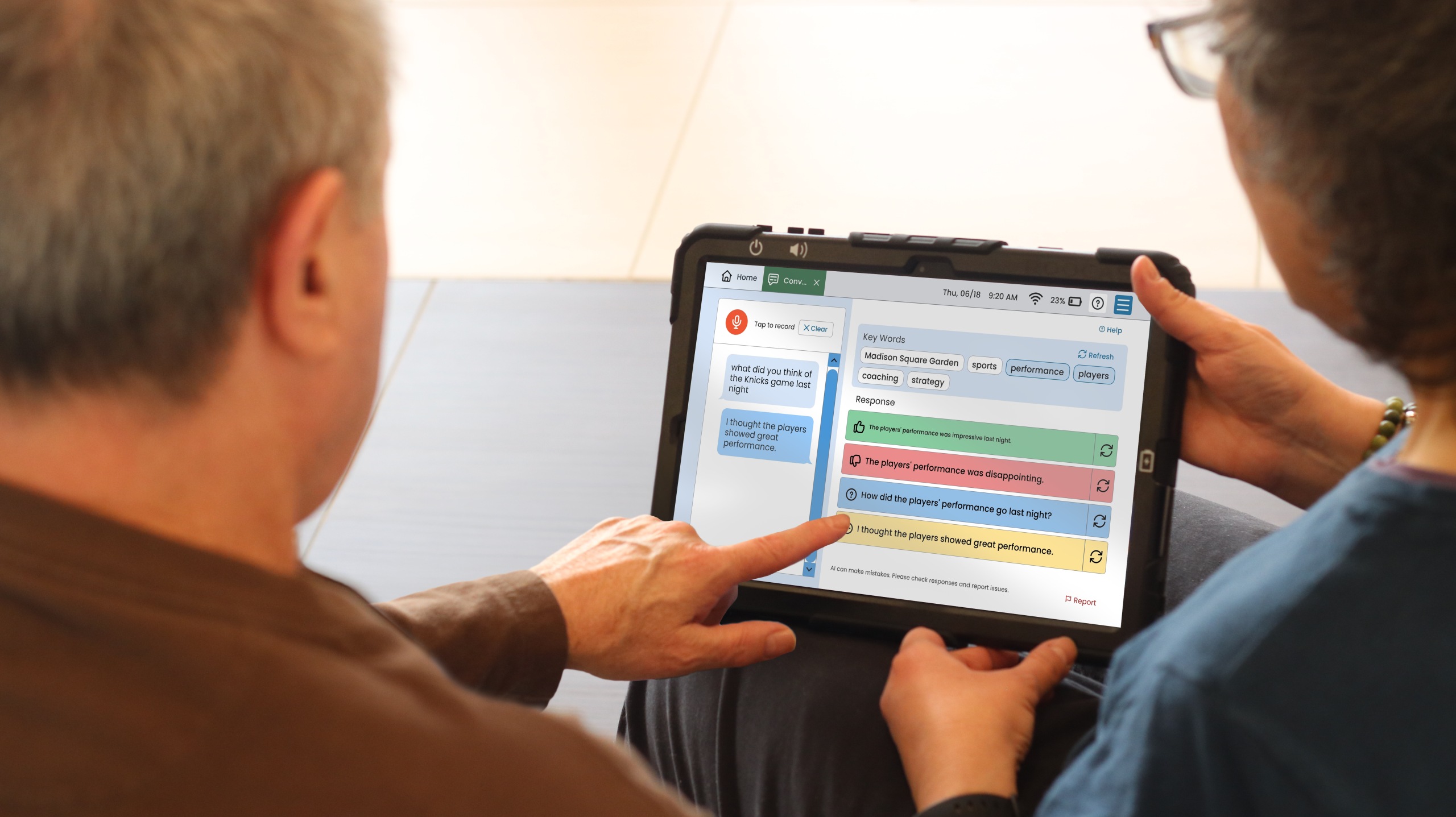
A meta-analysis by Kent-Walsh and colleagues (2015) found that successful device use depends on both the skills of the patient and the communication partner’s involvement.
What this means in practice:
- Communication partner modeling enhances AAC learning and use
- Partner training consistently improves communication outcomes
- Supported communication often achieves better functional results than independent attempts
- Environmental modifications and partner involvement are part of successful AAC implementation, not barriers to it
This research reframes support from a clinical deficit to a communication strength. When we view communication partners as essential components of successful AAC use rather than temporary scaffolds to be removed, we open up new possibilities for meaningful communication.
Where does support-based communication thrive?
Independence isn’t always possible, or even appropriate, across all situations and settings. Sometimes the idea of independence can actually miss the point.
Let’s zoom out and give several examples…
Clinical settings:
In acute care settings, patients need immediate communication access with medical staff for safety and care coordination. The focus should be on effective message transmission, not independent device mastery. Similarly, in long-term care facilities with high staff turnover and limited training time, supported communication approaches may be more realistic and effective than expecting independent use.
Individual factors:
Consider adults with progressive conditions like primary progressive aphasia (PPA), where abilities change over time. Expecting increasing independence doesn’t align with the nature of their condition. For individuals with complex medical needs, communication partners are essential for safety and comprehensive communication.
Environmental realities:
Real-world communication happens in noisy restaurants, dimly lit rooms, and busy medical appointments. Even neurotypical speakers rely on communication partners to repeat information, clarify messages, and provide context. Why, then, should AAC users be held to a different standard?
When we step back from independence as the primary benchmark, we can focus on what really matters: effective message transmission, reduced communication breakdowns, increased participation in meaningful activities, and enhanced quality of life and connection.
Other measures of AAC effectiveness
What would AAC success look like if we measured it differently?
Participation-based outcomes:
- Can the person engage in activities they value?
- Are they able to maintain important relationships?
- Do they have a voice in decisions that affect them?
- Has communication frustration decreased?
Functional communication measures:
- Are messages being understood by communication partners?
- Is communication happening efficiently in real-world contexts?
- Can the person communicate flexibly across different settings and partners?
- Does AAC integrate well with their existing communication methods?
Quality of life indicators:
- Does the person feel satisfied with their communication abilities?
- Do family members feel confident supporting communication?
- Has the communication burden on caregivers been reduced through effective AAC tools?
- Are dignity and autonomy maintained in communication choices?
These measures focus on communication effectiveness and life participation rather than the level of support required to achieve them.
For comprehensive guidance on setting meaningful AAC goals beyond independence, resources like Conquering AAC provide evidence-based frameworks for clinical practice.
Rethinking goals, documentation, and success metrics
How might our clinical practice change if we embraced a broader definition of AAC success?
Let’s look at the following 👇
Alternative goal writing:
Instead of “Patient will independently use AAC device,” consider:
- “Patient will communicate needs effectively using AAC with available support”
- “Patient will participate in conversations using multimodal communication approaches”
- “Communication partners will successfully support patient’s AAC use”
- “Patient will express preferences and make choices using AAC in preferred contexts”
Documentation focus:
Rather than tracking independence levels, document:
- Communication effectiveness across different contexts
- Environmental factors that support or hinder communication
- Partner involvement as a positive outcome, not a deficit
- Functional improvements in participation and quality of life
Clinical decision-making:
- Evaluate success based on functional communication outcomes
- Consider communication contexts and available supports as part of the intervention
- Include user and family perspectives on what constitutes meaningful communication
- Recognize that AAC devices are tools designed to work within support systems, not replace them
A more nuanced view of AAC success
Independence is one possible outcome for AAC use, but it shouldn’t be the only measure of success we value. Research consistently shows that communication partner involvement enhances AAC effectiveness, and real-world communication often requires environmental supports and collaborative interaction.
When we expand our definition of success beyond independence, we create space for more adults to benefit from AAC. We acknowledge the reality of how communication actually works in daily life, and we honor the important role that communication partners play in supporting meaningful interaction.
As you reflect on your current AAC users, ask this question:
What would success look like if independence wasn’t the primary benchmark?
The answer(s) might open up new possibilities for the adults you serve (and I bet they would love to tell you about it with their device!)
About Contributor
 Lauren Hermann, MS, CCC-SLP
Guest Contributor
Lauren Hermann, MS, CCC-SLP
Guest Contributor
Contributors
Lauren Hermann, MS, CCC-SLP
Guest Contributor
Categories
Subscribe to newsletter
Share